Bacterial STIs
Overview
About Bacterial STIs
Bacterial sexually transmitted infections (STIs) are a common public health concern. Whether “silent” or painful, these infections can have surprising long term health effects. Learning more about symptoms, complications, and prevention can equip people to make risk aware decisions and reduce negative outcomes.
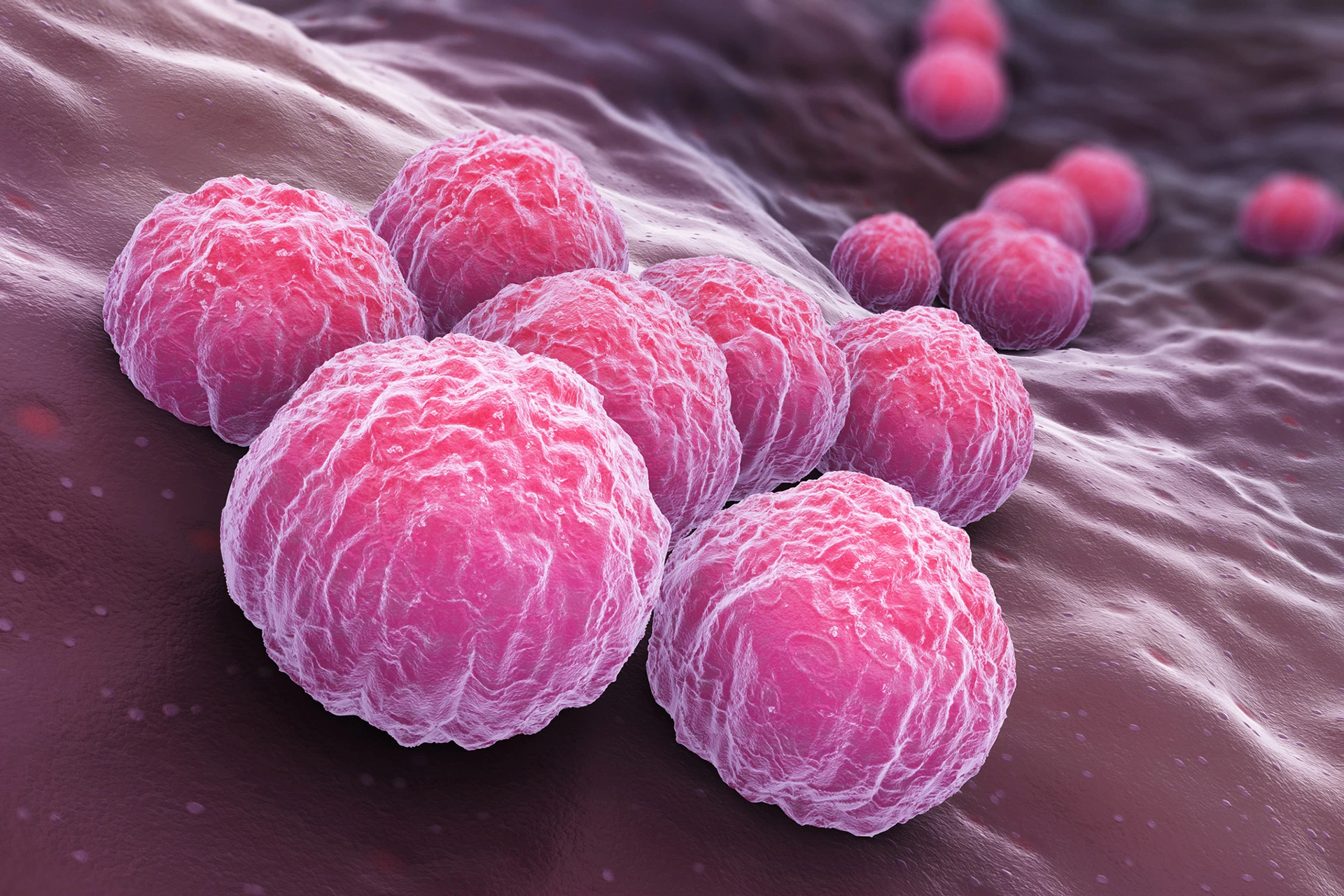
The most common bacterial STIs are chlamydia, gonorrhea, and syphilis. Other less common bacterial STIs include chancroid, mycoplasma genitalium, and granuloma inguinale. Bacterial vaginosis (BV) is considered a “sexually associated condition” in which the normal balance of bacteria in the vagina is disrupted. Treatment of sexual partners may be recommended with BV to help prevent re-occurrence.
These diseases are treated with one or multiple antibiotics and should include treatment for both the infected person and their sexual partners. Resistance to antibiotics is increasing, especially in cases of gonorrhea. Bacterial STIs cannot be prevented with vaccines.
Symptoms vary among bacterial STIs. Some are “silent”, without short-term manifestations. Others have bothersome symptoms.
Whether strong manifestations or none, many bacterial STIs are known to be risk factors for various types of cancer, infertility, or complications of pregnancy.
Prevention
Effective preventative measures include prevention of occurrence, early identification and treatment, and effective management of existing STIs.
Primary prevention includes encouraging abstinence from sexual activity outside of a long-term monogamous relationship, and avoidance of sex with infected persons. It also includes comprehensive education on STIs’ prevalence, deleterious short- and long-term effects, and the often asymptomatic (“silent”) nature. Finally, condom use with sexual activity should be encouraged but not primarily relied upon for prevention, as it reduces risk of acquiring non-viral STIs by only 59% (4).
Moreover, secondary prevention — screening and treating STIs early — is key to prevent transmission. Health care providers should screen at risk individuals, such as those with multiple sexual partners or men who have sex with men, and also pregnant women. They may test for chlamydia and gonorrhea with a simple urine test or vaginal or rectal swab. They may screen for syphilis with symptom identification and blood work.
Partners of those infected should also be screened and/or treated. Most states allow “expedited partner therapy”, in which a health care provider can prescribe STI treatment to an infected patient’s partner, without examination of the partner (2).
Finally, existing STIs should be managed effectively. Treatments should be according to latest guidelines and follow-up testing for reinfection or cure is often recommended.
In summary, bacterial STIs are common, treatable conditions with unwanted short- and long-term consequences. Screening and early treatment is key to preventing transmission. Avoidance of sexual activity outside of a long-term monogamous relationship is the most effective means of prevention.



Chlamydia
Overview
Chlamydia is a common bacterial STI that causes infections of the urethra, anus, or cervix. It can also cause more complicated infections, putting someone at risk for ectopic pregnancy or infertility.
Incidence
Chlamydia is the most common bacterial sexually transmitted infection (STI), affecting more than 1.5 million people in the U.S. in 2024 (CDC, 2025b). It is most common amongst teens and young adults. It is more common in women than men (CDC, 2023).
How Chlamydia Spreads
Chlamydia spreads by sex — including oral, vaginal, or anal sex (McCance, 2019). Consistent and correct condom use lowers someone’s chance of acquiring chlamydia from an infected person by 60% (Crosby et al., 2012).
Chlamydia can also transmit from a mom to baby during childbirth.
Types of Infections
Chlamydia most commonly infects the urethra of men and women and cervix of women. It can also travel up the reproductive tract to infect the epididymis in men (in the scrotum) and fallopian tubes of women.
Sometimes, it infects the anus and rectum.
Uncommon strains of chlamydia infect the eyes, or cause a serious disease called lymphogranuloma venereum.
Symptoms
Genital Infection
In women, symptoms of a chlamydia genital infection include vaginal discharge, urethral discharge, bleeding, or pain with urination (McCance, 2019). In men, infections present with penile discharge (clear, white, or grey), or mild pain with urination. Men may also experience pain in one or both scrotums.
More than half of genital chlamydial infections have no noticeable symptoms. (These infections are still contagious).
Anal Infection
If chlamydia affects the anus, someone may have rectal pain, bleeding, or discharge. This is most common if someone has anal sex and is the receptive partner.
Complications
Pelvic Inflammatory Disease & Infertility
The chlamydia bacteria may ascend into a woman’s fallopian tubes and ovaries, causing a serious disease called “pelvic inflammatory disease” (PID). Symptoms include abdominal pain, fever, and chills. This disease may cause permanent scaring and damage, making it harder or impossible to get pregnant (infertility). It may also cause ectopic pregnancy (pregnancy outside of the womb) — which is a life-threatening situation.
Cancer Risk
Chlamydia is a risk factor for cervical cancer, prostate cancer, ovarian cancer, and fallopian tube cancer (Poston, 2024).
Chlamydia and Newborns
In a newborn, chlamydia may cause eye infection (conjunctivitis) or pneumonia (McCance, 2019).
Diagnosis & Screening
A urine sample or sample from a vaginal, penile, or rectal swab is used to detect chlamydia (CDC, 2025a).
Screening
Health care providers may recommend being screened for an STI. This means being tested even when you have no symptoms. Risk factors include having multiple or new sex partners, having other STIs or a partner with an STI, history of incarceration, history of sex work, or inconsistent condom use (Davidson et al., 2021 & CDC, 2024b). All sexually active women younger than 25 and men who have sex with men are considered at risk and should be screened for chlamydia regularly.
Treatment
Chlamydia is treated with antibiotics (CDC, 2025a). Partners of infected persons should be treated as well. Sexual activity should be avoided until treatment is complete. Because reinfection is common, people who have completed treatment should be tested again 3 months after treatment is complete.
Prevention
Given the life altering complications of chlamydia — such as increased risk for PID, cancer, or infertility — prevention is key.
The best prevention is avoiding sex outside of a long term mutually faithful and monogamous relationship.
Other ways to reduce spread are using condoms correctly and consistently, having open and honest conversations about STIs with partners, and getting STI tested before sex.
Remember, chlamydia and other STIs may have no symptoms but can still spread.
Gonorrhea
Overview
Gonorrhea is a common bacterial STI that causes infections of the urethra, cervix, or anus. It can also cause more complicated infections, putting someone at risk for ectopic pregnancy or infertility.
Incidence
Gonorrhea effects more than 500,000 people in the U.S. in 2024 (CDC, 2025b). It is most common amongst men who have sex with men (MSM), followed by men who have sex with women, then women. Gonorrhea is most common in ages 20-24, and rates gradually decrease with age (CDC, 2023).
How Gonorrhea Spreads
Gonorrhea spreads by vaginal, anal, or oral sex. Condoms when used consistently and correctly, lower someone’s chance of acquiring gonorrhea by 60% (Crosby et al., 2012).
Gonorrhea also can transmit from mom to baby in childbirth.
Symptoms
Gonorrhea may have bothersome symptoms or no symptoms (McCance & Huether, 2019). Women are more likely to have no symptoms.
Genital Infection
Male symptoms include purulent penile discharge or pain with urination. Female symptoms include increased vaginal discharge or pain with urination or sex.
Rectal Infection
Rectal symptoms include rectal itching, pain, bleeding, or constipation.
Complicated Infection
Women may experience pelvic pain, fever, and excessive discharge as symptoms of pelvic inflammatory disease (PID). This occurs when gonorrhea spreads to other reproductive organs.
Men may experience pain in the scrotum or pelvic region while experiencing infections of the prostate or scrotum.
Complications
Pelvic Inflammatory Disease
Pelvic inflammatory disease occurs when gonorrhea spreads to upper reproductive organs in women, causing inflammation, pain, and often permanent damage. It increases a woman’s risk for infertility and ectopic pregnancy (pregnancy outside of the womb).
Epididymitis
Infection within the scrotum (epididymitis) increases a man’s risk for sterility.
Cancer Risk
Gonorrhea increases risk for bladder cancer and prostate cancer.
HIV Risk
Having gonorrhea increases risk of acquiring human immunodeficiency virus (HIV).
Bloodstream Infection
Rarely, gonorrhea may infect the bloodstream, causing serious complications such as joint pain or infection of the heart.
Gonorrhea and Newborns
In infants, Neisseria gonorrhoeae causes infection of the eyes (conjunctivitis), nose (rhinitis), or rectum (anorectal infection). It can cause blindness if treatment is delayed.
Diagnosis & Screening
Health care providers use a urine sample or sample from vaginal, penile, or rectal swab to detect gonorrhea.
Screening
Health care providers may recommend being screened for an STI. This means being tested even when you have no symptoms. Risk factors include having multiple or new sex partners, having other STIs or a partner with an STI, history of incarceration, history of sex work, or inconsistent condom use (Davidson et al., 2021 & CDC, 2024b). All sexually active women younger than 25 and men who have sex with men are considered at risk.
Treatment
Gonorrhea is treated with antibiotics. Gonorrhea has become resistant to many antibiotics, making treatment options limited. Partners of infected persons should also be tested and treated.
Those who are treated should wait one week until resuming sex to avoid infecting others (CDC, 2025a). The CDC recommends being tested again 3 months after treatment, because reinfection is common.
Prevention
Given the life altering complications of gonorrhea — such as increased risk for PID, prostatitis, or infertility — prevention is key.
The best prevention is avoiding sex outside of a long term mutually faithful and monogamous relationship.
Other ways to reduce spread are using condoms correctly and consistently, having open and honest conversations about STIs with partners, and getting STI tested before sex.
Remember, gonorrhea and other STIs may have no symptoms but can still spread.
Syphilis
Overview
Syphilis is a bacterial sexually transmitted disease (STI) that affects both adults and fetus/newborns (“congenital syphilis”). It is treatable with antibiotics. Timely treatment of the disease is critically important to prevent complications.
Incidence
186,000 cases of adult syphilis were reported in in the U.S. in 2024 (CDC, 2025c). More men than women are affected, and rates are highest among men who have sex with men (CDC, 2023). Young adults are most heavily affected.
Almost 4,000 cases of congenital syphilis were reported in the U.S. in 2024 (CDC, 2025b).
How Syphilis Spreads
Treponema pallidum, the bacteria that causes syphilis, spreads from an infected person to an uninfected person during sexual activity (CDC, 2025a & Tuddenham & Ghanem, 2019.
The disease spreads from chancres (sores) on the infected partner to minor cuts or areas of open skin on the uninfected partner. Body fluid may also be infectious if it comes in contact with a chancre.
Transmission can happen unknowingly, because chancres can be in unseen locations, such as inside the mouth or genitals, and cause no pain.
Additionally, syphilis may spread from an infected pregnant woman to her fetus through the placenta, as early as 9 weeks gestation (McCance & Huether, 2019).
Symptoms
Adult syphilis is categorized into four stages: primary, secondary, latent, and tertiary (CDC, 2025a & McCance & Huether, 2019). Symptoms vary in each stage. If untreated, the disease continues to progress through the stages.
Primary Stage
Primary syphilis presents as small (<2 cm) painless round sores at the site of exposure. Typically they are on or around the genitals or mouth. These sores resolve 2-8 weeks without treatment.
Secondary Stage
Secondary syphilis presents as a rash accompanied by mild to moderate generalized symptoms, such as headache, fatigue, body aches, low grade fever, and sore throat. The rash may affect the palms of hands or soles of feet. These symptoms occur about 6 weeks after initial sores (chancres).
Wart like, highly contagious lesions called condylomata lata may present on the perineum and vagina of women or surrounding the anus or inner thigh of men or women. These symptoms typically resolved after 2-10 weeks without treatment.
Latent Stage
Latent syphilis is a period in which the body suppresses the disease. Sores and systemic symptoms have resolved. It may last for many years.
Tertiary Stage
Tertiary syphilis typically occurs 10-30 years after the initial infection . Lesions called gummas may occur internally and externally. The disease may affect the heart and nervous system. Serious complications or death may occur.
Congenital Syphilis
Congenital syphilis is treatable, but delayed treatment or no treatment may cause grave complications.
Complications include prematurity, low birth weight, stillbirth, congenital abnormalities, or neonatal death. The mortality rate of congenital syphilis is approximately 31% (Wozniak et al., 2023).
A pregnant woman should be tested for syphilis at her first prenatal visit, in her third trimester, and at birth (ACOG, 2025). This allows timely treatment and minimizes risk of complications.
Complications
In addition to the complications of tertiary syphilis and congenital complications, syphilis may affect the eyes (ocular syphilis), ears (otosyphilis), or nervous system (neurosyphilis). This may lead to blindness, paralysis, dementia, and other complications.
Syphilis also increases risk of acquiring HIV due to the exposed skin at sores.
Screening
Health care providers may recommend being screened for syphilis. This means being tested even when you have no symptoms. Currently, the CDC and U.S. Preventative Task Force (USPTF) recommend that sexually active adults or teens with the following risk factors be screened: HIV, previous or current STI, history of incarceration, military service, sex work, or illicit drug use. (Mangione et al., 2022).
ACOG and the CDC pregnant women be screened at the first prenatal visit, in the third trimester, and at birth (ACOG, 2025).
Diagnosis
Syphilis is diagnosed through a two-part blood test. The nontreponemal antigen tests (RPR and VDRL) are used for initial screening, and a treponemal test is used for conclusive diagnosis.
Treatment
Syphilis is treated with antibiotics. Repeat testing to confirm successful treatment is recommended. Partners should also be tested and treated.
Prevention
Prior to sexual activity, both partners should have an open and honest discussion about past or present STIs, and be tested for STIs if at risk (for example multiple past sexual partners).
It is important to note that chancres (sores) from syphilis can be in unseen locations, such as inside the mouth or near the cervix.
The best way to avoid acquiring an STI is only being sexually active within a long term mutually monogamous relationship.
Condoms do not prevent syphilis unless the condom covers all sores.
Mycoplasma Genitalium (Mgen)
Overview
Mycoplasma genitalium, or Mgen, is a sexually transmitted infection (STI) that causes urinary and genital symptoms and reproductive complications if untreated. It is caused by a slow growing bacteria and is treated with antibiotics.
Incidence
Mgen affects both men and women. It is more common amongst those with multiple sexual partners.
How Mgen Spreads
Mgen spreads by having vaginal or anal sex with an infected person. Someone with no symptoms may still pass on the infection to others. It may also spread by oral sex, but this data is not yet available.
Symptoms (Excluding Congenital)
Women
Mgen can cause cervicitis (inflammation of lower portion of the uterus or “womb”). Symptoms of cervicitis include vaginal discharge, odor, bleeding between periods, or pain with sex.
Mgen infections can also extend upwards into the uterus and fallopian tubes, leading to Pelvic Inflammatory Disease (PID). Symptoms of PID include fever, chills, abdominal pain, abnormal vaginal bleeding or odor.
Men
Mgen may cause urethritis, leading to abnormal penile discharge or pain with urination.
Rectal Symptoms
In both men and women, Mgen can infect the rectum, leading to “proctitis”. Symptoms of proctitis include rectal bleeding, pain with bowel movements, abnormal bowel movements, or abnormal rectal discharge.
Diagnosis
A health care provider may diagnose Mgen through testing urine or swab of vagina, cervix, or penis.
Treatment
Mgen is treated with antibiotics as directed by the CDC. Mgen is resistant to some antibiotics and may require multiple antibiotics.
Complications
Like many STIs, Mgen increases the risk of acquiring or spreading HIV.
It also increases the risk of infertility, preterm delivery, ectopic pregnancy, or other birth complications.
Some cases of Mgen are resistant to first line treatments (antibiotic resistance). These infections are treated with additional antibiotics.
Prevention
As with other STIs, Mgen can be prevented by avoiding sex with an infected person. The more sexual partners, the higher the risk of acquiring an STI. Having sex within a long term mutually monogamous relationship, where both partners have been tested and treated for STIs, is the best way to avoid an STI.
Using condoms consistently and correctly reduces the risk of acquiring Mgen. Someone with Mgen should take antibiotics as prescribed and return to a health care provider if symptoms do not improve.
Last updated on May 7, 2026
In the News


References
1Centers for Disease Control and Prevention. (2024, February 15). Drug – Resistant Gonorrhea. https://www.cdc.gov/gonorrhea/hcp/drug-resistant/index.html
2Centers for Disease Control and Prevention. (2024, July 16). Expedited Partner Therapy. https://www.cdc.gov/sti/hcp/clinical-guidance/expedited-partner-therapy.html
3Centers for Disease Control and Prevention. (2024, April 3). Sexually Transmitted Infections Prevalence, Incidence, and Cost Estimates in the United States. https://www.cdc.gov/sti/php/communication-resources/prevalence-incidence-and-cost-estimates.html
4Crosby, R. A., Charnigo, R. A., Weathers, C., Caliendo, A. M., & Shrier, L. A. (2012). Condom effectiveness against non-viral sexually transmitted infections: a prospective study using electronic daily diaries. Sexually transmitted infections, 88(7), 484–489. https://doi.org/10.1136/sextrans-2012-050618
5McCance, K.L., & Huether, S.E. (2019). Sexually transmitted infections. In V.L. Brashers & N.S. Rote (Eds.), Pathophysiology: The biologic basis for disease in adults and children (pp 869-879). Elsevier.
Chlamydia References
Alexiou, Z. W., Hoenderboom, B. M., Hoebe, C. J., Dukers-Muijrers, N. H., Götz, H. M., van der Sande, M. A., … & van Benthem, B. H. (2024). Reproductive tract complication risks following Chlamydia trachomatis infections: a long-term prospective cohort study from 2008 to 2022. The Lancet Regional Health–Europe, 45.
Centers for Disease Control and Prevention. (2025a, January). About Chlamydia. https://www.cdc.gov/chlamydia/about/index.html
Centers for Disease Control and Prevention. (2024, March 22). Screening Recommendations and Considerations Referenced in Treatment Guidelines and Original Sources. https://www.cdc.gov/std/treatment-guidelines/screening-recommendations.htm
Centers for Disease Control and Prevention. (2023). Sexually transmitted infections surveillance 2023. https://www.cdc.gov/sti-statistics/media/pdfs/2025/09/2023_STI_Surveillance_Report_FINAL_508.pdf
Centers for Disease Control and Prevention. (2025b, September 24). Sexually Transmitted Infections Surveillance, 2024 (Provisional). https://www.cdc.gov/sti-statistics/annual/index.html
Crosby, R. A., Charnigo, R. A., Weathers, C., Caliendo, A. M., & Shrier, L. A. (2012). Condom effectiveness against non-viral sexually transmitted infections: a prospective study using electronic daily diaries. Sexually transmitted infections, 88(7), 484–489. https://doi.org/10.1136/sextrans-2012-050618
Davidson, K. W., Barry, M. J., Mangione, C. M., Cabana, M., Caughey, A. B., Davis, E. M., … & US Preventive Services Task Force. (2021). Screening for chlamydia and gonorrhea: US Preventive Services Task Force recommendation statement. Jama, 326(10), 949-956.
McCance, K.L., & Huether, S.E. (2019). Sexually transmitted infections. In V.L. Brashers & N.S. Rote (Eds.), Pathophysiology: The biologic basis for disease in adults and children (pp 877-878). Elsevier.
Poston, T. B. (2024). Advances in vaccine development for Chlamydia trachomatis. Pathogens and Disease, 82, ftae017.
Gonorrhea References
Centers for Disease Control and Prevention. (2025a, January 31). About Gonorrhea. https://www.cdc.gov/gonorrhea/about/index.html
Centers for Disease Control and Prevention. (2024, February 15). Drug – Resistant Gonorrhea. https://www.cdc.gov/gonorrhea/hcp/drug-resistant/index.html
Centers for Disease Control and Prevention. (2023). Sexually transmitted infections surveillance 2023. https://www.cdc.gov/sti-statistics/media/pdfs/2025/09/2023_STI_Surveillance_Report_FINAL_508.pdf
Centers for Disease Control and Prevention. (2025b, September 24). Sexually Transmitted Infections Surveillance, 2024 (Provisional). https://www.cdc.gov/sti-statistics/annual/index.html
Crosby, R. A., Charnigo, R. A., Weathers, C., Caliendo, A. M., & Shrier, L. A. (2012). Condom effectiveness against non-viral sexually transmitted infections: a prospective study using electronic daily diaries. Sexually transmitted infections, 88(7), 484–489. https://doi.org/10.1136/sextrans-2012-050618
Davidson, K. W., Barry, M. J., Mangione, C. M., Cabana, M., Caughey, A. B., Davis, E. M., … & US Preventive Services Task Force. (2021). Screening for chlamydia and gonorrhea: US Preventive Services Task Force recommendation statement. Jama, 326(10), 949-956.
McCance, K.L., & Huether, S.E. (2019). Sexually transmitted infections. In V.L. Brashers & N.S. Rote (Eds.), Pathophysiology: The biologic basis for disease in adults and children (pp 869-872). Elsevier.
Syphilis References
American College of Obstreticians and Gynecologists. (2025, October). Screening for Syphilis in Pregnancy. https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2024/04/screening-for-syphilis-in-pregnancy
Centers for Disease Control and Prevention. (2025a, January 30). About Syphilis. https://www.cdc.gov/syphilis/about/index.html
Centers for Disease Control and Prevention. (2025b, January 31). About Congenital Syphilis. https://www.cdc.gov/syphilis/about/about-congenital-syphilis.html
Centers for Disease Control and Prevention. (2023). Sexually transmitted infections surveillance 2023. https://www.cdc.gov/sti-statistics/media/pdfs/2025/09/2023_STI_Surveillance_Report_FINAL_508.pdf
Centers for Disease Control and Prevention. (2025c, September 24). Sexually Transmitted Infections Surveillance, 2024 (Provisional). https://www.cdc.gov/sti-statistics/annual/index.html
Mangione, C. M., Barry, M. J., Nicholson, W. K., Cabana, M., Chelmow, D., Coker, T. R., … & US Preventive Services Task Force. (2022). Screening for syphilis infection in nonpregnant adolescents and adults: US Preventive Services Task Force reaffirmation recommendation statement. Jama, 328(12), 1243-1249.
McCance, K.L., & Huether, S.E. (2019). Sexually transmitted infections. In V.L. Brashers & N.S. Rote (Eds.), Pathophysiology: The biologic basis for disease in adults and children (pp 872-875). Elsevier.
Silverstein, M., Wong, J. B., Davis, E. M., Chelmow, D., Coker, T. R., Fernandez, A., … & US Preventive Services Task Force. (2025). Screening for syphilis infection during pregnancy: US Preventive Services Task Force reaffirmation recommendation statement. JAMA, 333(22), 2006-2012.
Tuddenham, S., & Ghanem, K. G. (2019). What Is the Evidence for the Sexual Transmission of Syphilis From Asymptomatic Persons?. Sexually transmitted diseases, 46(6), e60–e61. https://doi.org/10.1097/OLQ.0000000000000987
Wozniak, P. S., Cantey, J. B., Zeray, F., Leos, N. K., Michelow, I. C., Sheffield, J. S., Wendel, G. D., & Sánchez, P. J. (2023). The Mortality of Congenital Syphilis. The Journal of pediatrics, 263, 113650. https://doi.org/10.1016/j.jpeds.2023.113650
Mycoplasma Genitalium References
Centers for Disease Control and Prevention. (2021, July 22). Sexually transmitted infections treatment guidelines, 2021: Mycoplasma genitalium. https://www.cdc.gov/std/treatment-guidelines/mycoplasmagenitalium.htm
Centers for Disease Control and Prevention. (2025, January 31). About Mycoplasma genitalium. https://www.cdc.gov/mgen/about/index.html
Htaik, K., Vodstrcil, L. A., Plummer, E. L., Sfameni, A. M., Machalek, D. A., Manhart, L. E., & Bradshaw, C. S. (2024). Systematic review and meta-analysis of the association between Mycoplasma genitalium and pelvic inflammatory disease (PID). Clinical Infectious Diseases, ciae295.
McCullough, A., & Palokas, M. (2024). Prevalence and incidence of Mycoplasma genitalium infection: a systematic review protocol. JBI Evidence Synthesis, 22(4), 700-705.
Mycoplasma genitalium infections. Infectious Disease Clinics of North America, 37(2), 311-333.
Wood, G. E., Bradshaw, C. S., & Manhart, L. E. (2023).